

Mr Tanner has advised you to have retinal detachment surgery. This leaflet gives you information that will help you decide what to do. You may wish to discuss the information with a relative or carer. Before you have the operation, he will ask you to sign a consent form, so it is important that you understand the information in this leaflet.
You have been diagnosed with a retinal detachment in your eye. Without treatment, this condition usually leads to blindness in the eye affected. The retina is a thin layer of nerve cells that lines the inside of the eye. It is sensitive to light (like the film in a camera) and you need it to be able to see.
Your retina is detached because it has one or more holes in it. These holes allow fluid to pass beneath the retina, causing separation from the underlying, supporting and nourishing tissues. You may have some bleeding into the vitreous (the jelly substance in the centre of the eye), causing further clouding of the vision.
Retinal detachments happen naturally. It is unlikely that it would be caused by anything you have done. Anyone can develop a retinal detachment at any time, but certain people are at a higher risk than others. These include people who are short sighted, those who have had cataract surgery in the past, and those who have recently suffered a severe blow to the eye. Some types of retinal detachments can run in families, but these are rare.

The treatment involves surgery. During the operation, Mr Tanner will seal the retinal holes and re-attach your retina.
Patients have a choice of either general or local anaesthetic. If having a general anaesthetic you will be asked not to eat or drink for several hours before we take you to the operating theatre.
Before the operation, an anaesthetist will speak to you and examine you on the ward.
Before the operation, we will give you eye drops to enlarge your pupils. You may feel tired and sleepy for about six to twelve hours after the operation. Your good eye is often examined while you are asleep to ensure it is healthy and to give you protective treatment, if necessary. This may mean that both eyes are red and uncomfortable after the surgery.
There are many types of surgery. We can seal the retinal holes by applying supports on the wall of the eye. These supports are made of sponge or solid silicone material. We put them under the covering of the eye (conjunctiva), and they usually stay there permanently. Other people will not usually notice them.
In some cases, the jelly-like substance called the vitreous, needs to be removed. This is called vitrectomy. During this operation, Mr Tanner will make three needle-sized holes in the eye and remove the vitreous, replacing it with a gas or liquid silicone oil bubble.
This bubble acts as a support to hold the retina in position to help it to heal. If we use a gas, your normal body fluids will replace it naturally over time. If we use silicone, we may need to remove this with another operation several months after your first operation.
We usually put small stitches in the eye. At the end of the operation, we may put a pad or bandage over your eye to protect it and reduce swelling.
If you have discomfort, we suggest that you take a pain reliever, such as paracetamol, every four to six hours. It is normal to feel itching, sticky eyelids and mild discomfort for a while after retinal detachment surgery. It is common for your eye to water. Occasionally, the area surrounding the eye can become bruised. Any discomfort should ease after two to three days. In most cases, your eye will take about six weeks to heal. You will normally see Mr Tanner in the clinic one to two weeks after your operation. Try to rest while your eye is healing.
We will give you eye drops to reduce any inflammation, to rest the eye and to prevent infection. We will explain how and when you should use them. Please do not rub your eye.
Certain symptoms could mean that you need prompt treatment. Please contact Mr Tanner or the local eye casualty immediately if you have any of the following symptoms:
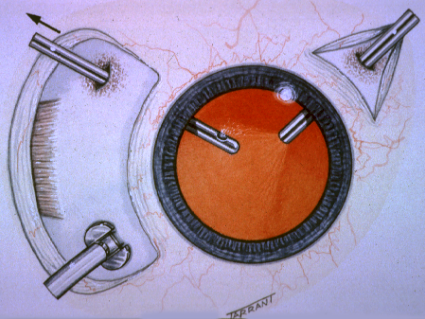

Per-operative photograph of vitrectomy for retinal detachment
If you have discomfort, we suggest that you take a pain reliever, such as paracetamol, every four to six hours. It is normal to feel itching, sticky eyelids and mild discomfort for a while after retinal detachment surgery. It is common for your eye to water. Occasionally, the area surrounding the eye can become bruised. Any discomfort should ease after two to three days. In most cases, your eye will take about six weeks to heal. You will normally see Mr Tanner in the clinic one to two weeks after your operation. Try to rest while your eye is healing.
We will give you eye drops to reduce any inflammation, to rest the eye and to prevent infection. We will explain how and when you should use them. Please do not rub your eye.
Certain symptoms could mean that you need prompt treatment. Please contact Mr Tanner or the local eye casualty immediately if you have any of the following symptoms:
If Mr Tanner puts a gas or silicone bubble in the eye, he will usually ask you to keep your head and body in a particular position. This is called ‘posturing’ and aims to provide support to seal the holes in the retina. The bubble floats inside the eye cavity and we will usually ask you to hold your head in a position so that the bubble lies against the holes. This is an important part of the treatment and the position you hold your head in will depend on where the holes are in your retina. We may also advise you to sleep in a certain position at night. By following the instructions, you will give your retina the best chance to be successfully treated. Your co-operation matters a great deal.
When you have a gas bubble in your eye, you must not travel by aeroplane.
Retinal detachment surgery endeavours to prevent you from going blind and help you see more clearly. You have already lost some sight. If the surgery is successful, it will usually bring back some, but not all of your sight.
Retinal detachment surgery is not always successful. Every patient is different. Detached retinas are complicated to treat. Some patients may need more than one operation. Mr Tanner will talk to you about the chances of success in your particular case. Unfortunately, in difficult cases, vision can be lost following retinal surgery. However, without surgery the majority of eyes would definitely lose vision.
There is a risk of complications, either during or after the operation. Minor complications are common and in most cases we can treat them effectively. Very rarely, some complications can result in blindness.
Possible complications during the operation:
Possible complications after the operation:
If the first operation is not successful, you will need to have more surgery. If you have a vitrectomy to repair your retinal detachment, you will probably require cataract surgery 6-12 months following your retinal surgery.
Mr Tanner will be happy to answer any further questions you may have.
Disclaimer : The information provided in this website is intended as a useful aid to general practitioners, optometrists and patients. It is impossible to diagnose and treat patients adequately without a thorough eye examination by a qualified ophthalmologist, optometrist or your general practitioner. Hopefully the information will be of use prior to and following a consultation which it supplements and does not replace.
